
What it is
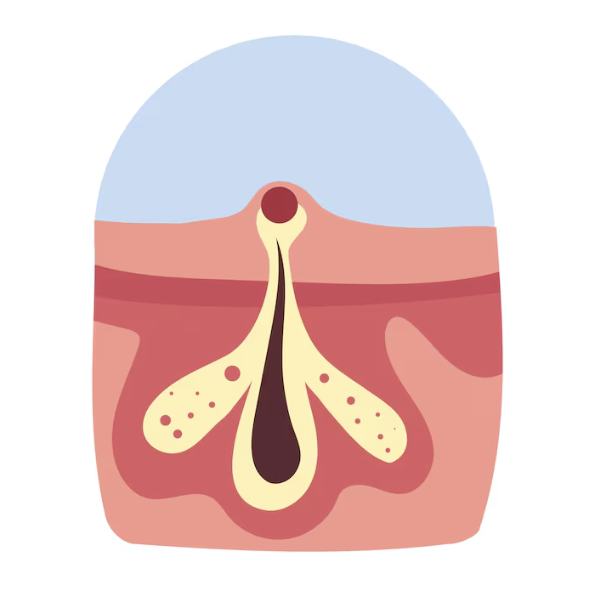
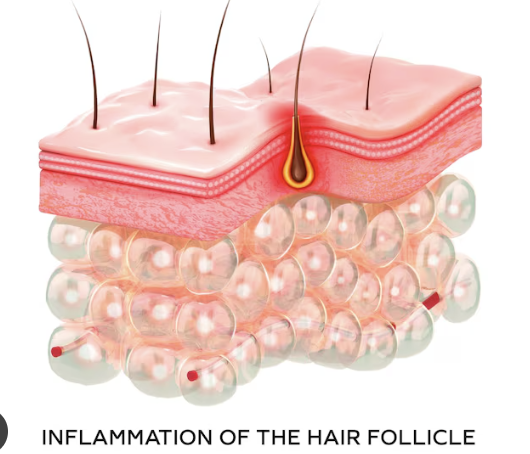
Folliculitis is inflammation that centers on a hair follicle. It can be bacterial, fungal, viral — or have nothing to do with infection at all.
That's why a breakout that looks like acne might need antibiotics, antifungals, antivirals, a change in how you shave, or no antimicrobial treatment whatsoever. The cause dictates the cure — and that cause is often invisible without paying close attention to where, when, and how the bumps appeared.

What folliculitis looks like
The classic lesion is a small bump or pustule sitting right at the base of a hair, often with a faint ring of redness around it. Bacterial cases tend to be tender; yeast cases tend to be itchy; viral cases can hurt before they ever blister.

Location is a powerful clue. Beard-area bumps after shaving point one direction; itchy, uniform bumps across the upper back point somewhere else entirely; pustules confined to the swimwear zone after a hot tub point at a third diagnosis altogether.

Why it gets confused with acne
- Comedones (blackheads & whiteheads)
- Mixed papules, pustules, nodules
- Pilosebaceous-unit disorder
- No comedones (usually)
- Uniform, hair-centered bumps
- Often itchy or tender
The single most useful question is: are there comedones? If yes, acne is far more likely. If no — and especially if antibiotics have already failed — yeast or another folliculitis enters the running.
The major types
Each one has a signature presentation and a different treatment path. Recognizing the pattern saves weeks of trial-and-error.

Bacterial
Tell-tale clue: Tender pustule sitting on a hair follicle, ringed by a halo of redness. Can deepen into a boil if ignored.
Direction of treatment: Antiseptics, topical or oral antibiotics, drainage for boils.

Hot-tub
Tell-tale clue: Itchy bumps appearing 1–2 days after a soak — concentrated under swimwear, on hips, back, or buttocks.
Direction of treatment: Usually self-resolves in 7–14 days. Antipseudomonal therapy if severe.

Malassezia
Tell-tale clue: Itchy, uniform tiny papules on chest, back, shoulders, hairline. Crucially: no comedones (blackheads/whiteheads).
Direction of treatment: Topical or oral antifungals — antibiotics make it worse.
Viral (HSV / VZV)
Tell-tale clue: Acute, painful, sometimes dermatomal lesions. Classic vesicles may be missing — diagnosis often needs PCR.
Direction of treatment: Clinician-directed antivirals, urgent if near the eye.

Pseudofolliculitis barbae
Tell-tale clue: Bumps, dark spots, and tenderness in shaved areas — especially in coarse or curly hair after close shaves.
Direction of treatment: Change the shave: clippers, with-the-grain, no skin-stretch.

Sterile / drug-related
Tell-tale clue: Eosinophilic, keloidal, actinic, or medication-triggered eruptions that defy antibiotics & antifungals.
Direction of treatment: Identify the trigger, treat the underlying disorder, dermatology referral.
Folliculitis on the scalp


At-a-glance comparison
| Type | Cause | Typical clue | Triggers | Treatment |
|---|---|---|---|---|
| Bacterial | Usually S. aureus | Tender follicular pustules, perifollicular redness, may form boils | Shaving, friction, trauma, S. aureus carriage | Antiseptics, topical/oral antibiotics, culture, incision & drainage |
| Hot-tub | Pseudomonas aeruginosa | Pustules in swimwear distribution after warm-water exposure | Hot tubs, whirlpools, biofilms, prolonged wet occlusion | Self-limited; antipseudomonal antibiotics for severe / immunocompromised |
| Malassezia | Malassezia yeast overgrowth | Itchy, uniform follicular papules on chest, back, hairline — no comedones | Heat, sweat, occlusion, antibiotics, steroids | Topical antifungals, antifungal washes, oral antifungals |
| Viral (HSV / VZV) | Herpes simplex or varicella-zoster | Painful, acute, dermatomal — vesicles may be absent | Reactivation, immunosuppression, atypical presentations | Viral testing + clinician-directed antiviral therapy |
| Pseudofolliculitis barbae | Ingrown hairs after shaving | Papules, pustules, hyperpigmentation in shaved areas | Curly/coarse hair, close shaves, blunt blades, against grain | Modify shaving, clippers, keratolytics, retinoids, laser hair reduction |
Risk factors & triggers

Shaving, waxing, plucking
Hair removal injures follicles, spreads bacteria, and traps regrowing hairs.
Try this → Pause hair removal during flares. Use clippers. Shave with the grain — never stretch the skin.
Sweat, humidity, heat
Creates the warm, occluded environment Malassezia thrives in.
Try this → Shower after heavy sweating. Change out of damp clothes promptly.
Antibiotic exposure
Disrupts the skin microbiome and is repeatedly linked to yeast folliculitis.
Try this → If acne worsens after antibiotics, suspect Malassezia and rethink the diagnosis.
Tight clothing & occlusion
Heavy oils and synthetic fabrics seal in heat and irritate follicles.
Try this → Choose breathable cotton or linen. Skip heavy occlusive products on prone zones.
Hot tubs & wet swimwear
Warm water + biofilm = Pseudomonas territory.
Try this → Shower & change immediately after a soak. Wash swimwear after every use.
Steroids & immunosuppression
Increases risk of atypical, viral, eosinophilic, or drug-related eruptions.
Try this → Seek earlier evaluation when lesions are unusual, recurrent, or treatment-resistant.
Treatment principles
Bacterial folliculitis
Mild superficial cases may resolve on their own in 7–10 days. Topical antibiotics like clindamycin or mupirocin and antiseptics like benzoyl peroxide are common first steps. Systemic antibiotics are reserved for extensive disease or systemic signs. Boils and abscesses often need drainage — not just antibiotics.
Antifungal direction
Malassezia folliculitis usually needs antifungals — the very thing acne antibiotics don't provide. Topical antifungals, ketoconazole washes, or oral antifungals are typical, with maintenance therapy because relapse is common.
Viral direction
Suspect HSV or VZV when lesions are acute, painful, dermatomal, or unresponsive to antibacterials and antifungals. PCR or biopsy may be needed. Antiviral therapy is critical when the eye is involved or the patient is immunocompromised.
Pseudofolliculitis barbae
The cure is mechanical, not pharmaceutical. Use clippers leaving 1+ mm of hair, hydrate before shaving, shave with the grain, and don't stretch the skin. Keratolytics or laser hair reduction help in stubborn cases.
Common mimics
Several conditions share the same general look. These are the ones most likely to throw off a quick visual diagnosis.
Acne vulgaris+
Clue · Comedones (blackheads/whiteheads) plus inflammatory bumps.
What sets it apart · The presence of comedones strongly favors acne over folliculitis.
Rosacea+
Clue · Central facial redness, flushing, telangiectasias, papules — no comedones.
What sets it apart · Background flushing is more typical than follicle-centered pustules.
Keratosis pilaris+
Clue · Tiny rough keratotic bumps, usually painless.
What sets it apart · Chronic, rough, sandpaper-like — not pustular or infectious-looking.
Molluscum contagiosum+
Clue · Smooth, dome-shaped papules with a central dimple (umbilication).
What sets it apart · The umbilication is the giveaway — bacterial / yeast folliculitis lacks it.
Prevention strategies
If shaving triggers it
- Switch to electric clippers leaving 1mm of stubble
- Hydrate the area with warm water first
- Always shave with the grain
- Replace blades often — sharpness matters
If sweat & heat trigger it
- Shower promptly after exercise
- Skip heavy occlusive products on prone zones
- Choose breathable fabrics
- Discuss antifungal washes with a clinician
If hot tubs trigger it
- Shower & change immediately after a soak
- Wash swimwear after every use
- Avoid poorly maintained spas
- Skip warm water entirely during a flare
If antibiotics keep failing
- Reconsider the diagnosis — likely Malassezia
- Stop empiric antibiotic cycles
- Ask for KOH or microscopy
- Try an antifungal trial under clinician guidance
When to see a doctor
Don't wait it out if…
- lesions are spreading rapidly or very painful
- you have fever, chills, or expanding redness
- a bump turns into a boil or abscess
- the eruption is near the eye
- lesions scar or cause hair loss
- you're immunocompromised, diabetic, or on cancer therapy
- the rash keeps coming back despite treatment

Quick pattern checklist
References
- Chiriac A, et al. Folliculitis: recognition and management. PubMed.
- Nomura T, et al. Special types of folliculitis which should be differentiated from acne. PubMed Central.
- Leung AKC, et al. Dermatology: how to manage acne vulgaris. PubMed Central.
- Del Giudice P. Skin Infections Caused by Staphylococcus aureus. PubMed Central.
- Chi CC, et al. Interventions for bacterial folliculitis and boils. PubMed Central.
- Chalupczak E, Lipner SR. Malassezia Folliculitis: An Underdiagnosed Mimicker of Acneiform Eruptions. PubMed Central.
- Saunte DML, et al. Position statement: recommendations for the diagnosis and treatment of Malassezia folliculitis. PubMed.
- Feschuk AM, et al. Clinical characteristics and treatment outcomes of Pityrosporum folliculitis in immunocompetent patients. PubMed Central.
- Jacob JS, Tschen JA. Hot Tub-Associated Pseudomonas Folliculitis. PubMed Central.
- Berger RS, Seifert MR. Whirlpool folliculitis: a review of its cause, treatment, and prevention. PubMed.
- Silverman AR, Nieland ML. Hot tub dermatitis: a familial outbreak of Pseudomonas folliculitis. PubMed.
- Ratnam S, et al. Pseudomonas folliculitis: a complication of the recreational use of contaminated waters. PubMed.
- Ogunbiyi A. Pseudofolliculitis barbae; current treatment options. PubMed Central.
- Alexis AF, et al. A Review of the Current Literature of Therapeutic Options for Pseudofolliculitis Barbae. PubMed.
- Cao X, et al. Facial Herpetic Folliculitis Should Be Concerned in the Clinic. PubMed Central.
- Boer A, et al. Herpes folliculitis: clinical, histopathological, and molecular pathologic observations. PubMed.
- Rogers RS, et al. Herpetic zoster folliculitis in the immunocompromised host. PubMed Central.
- Dodiuk-Gad RP, et al. Herpes folliculitis. PubMed.
- Kim JE, et al. Comparison between Malassezia folliculitis and non-Malassezia folliculitis. PubMed Central.
- Ogawa M, et al. Eosinophilic Pustular Folliculitis Associated with Herpes Zoster. PubMed.
Imagery in this article is sourced from Unsplash and Pexels and used under their respective free-use licenses. Photographs are illustrative; they do not depict diagnostic specimens.
This guide is for education. It cannot replace an in-person exam, culture, biopsy, or prescription. If something on your skin is painful, spreading, recurrent, or simply not improving — please talk to a clinician.